3. Joint injuries
Certain injuries hinder the athlete’s activity for quite a long time, and most of these injuries are joint injuries. Joint injuries are among the nightmares of athletes and coaches because they are difficult and slow to heal due to the fact that the regeneration time of the joint – due to its histological characteristics – is much longer than that of the muscles: while a muscle can recover in days or weeks, complete healing of a more severely injured joint may take a half to one year, if it is even able to heal completely at all (see, for example, Loitz, Frank 1993; Gabriel 2002).
The spontaneous, natural healing process of serious injuries goes through three basic phases:
bleeding and inflammation
the formation of molecular and cellular bridges between the ripped edges (repair phase) and then
remodelling.
The inflammatory phase lasts for about three days, the repair phase from two days to six weeks (the collagen synthesis rate usually reaches its peak three weeks after the injury), while the remodelling lasts from about one or one and a half months to a half or one year (Oakes 1992, Gabriel 2002). Missing out basic steps in treatment, such as resting, ice-packing, compression, and elevation (RICE), may result in excessive bleeding and edema, preventing the normal arrangement of collagen fibres, which results in the resulting scar tissue being too rigid, brittle, thick and painful (Gabriel 2002).
It should be noted that, in the event of a rupture of the articular ligament, early mobilization (i.e. within the first three weeks) may also interfere with the correct orientation of the collagen fibres, but after three weeks it is advisable to move and exert a fine load because this strengthens the healing ligaments (Gabriel 2002).
Of course not all joints and joint components react equally to the injury. For example, the knee joint’s medial collateral ligament, going through the appropriate treatment phases, has a fairly good healing potential even in the event of a complete tear, while, for example, in the same joint, when the anterior cruciate ligament is torn, the outlook is much worse, probably due to the exposure of the torn ligament edges to the synovial fluid (Gabriel 2002).
3.1. Injury due to overuse
Overload injuries are basically the result of cumulative microtrauma. These tiny injuries require regeneration, but if we do not allow time and opportunity, for example, because they are not even noticed, then the negative effects will accumulate and eventually result in injury. In the healing phase of these injuries, it is very likely that re-injury cycles may occur because the athlete does not detect or take seriously the recommended waiting time for the healing phase, and as the pain has passed, s/he resumes the load. This behaviour is triggered by a completely natural physiological and psychological phenomenon. The behaviour stems from the fact that as the athlete reaches an ever higher and stronger level in the given activity, the energy that s/he has to devote to further development is disproportionately increased, so the development over time shows a rough saturation curve. In fact, a lot of energy is simply needed to maintain the established level. On the one hand, this will result in an unpleasant feeling after recovering from injury, when the athlete sees how much he/she has regressed compared to the performance of the period before the injury, and on the other hand it is also physically difficult to get back to the previous level. That’s why many athletes do anything to fall back less, and get back to “their old selves” more easily. So it is easy to understand that the cessation of the pain is felt to be equivalent to the injury healing, and so the athlete resumes training with great intensity, which can, of course, cause further injury.
One very important reason why the joints are repeatedly injured is that the joint’s adaptability is much more limited and slower than that of the muscle. That is why many athletes experience the phenomenon that while their muscles grow and strengthen, during the rather rapid transformations – sometimes lasting as little as a few weeks – they believe that, for a sustained development, the load can be increased at the same pace as before. However, this is not the case. The adaptation of the joints occurs much more slowly, and unfortunately the athlete is not able to perceive this process as tangibly as with muscle development. Therefore, he/she is enthusiastic about the “surge” in muscle development, and – too focused on muscle development – forgets that there are also other components of the locomotor system, not just the muscles. Good coaches pay attention that their athletes do not go overboard to increase their load, carried away by the visible growth of their muscles. This effect is particularly dangerous for men, because in their body male hormones cause, a priori, a larger average increase in muscle protein synthesis than is the case for women; and since large muscles are usually an important component of the image of masculinity, they are less inclined to resist the temptation of excessively paced training plans, enticed by the promise of rapid development, but often ending up with joint injuries.
In addition, these injuries may not necessarily always occur where we would expect them from the way the limb is loaded. For example, in a substantial part of the training plans of short-distance runners, roughly half of the training sessions are technical running and the other half are strength training sessions, as a strong upper body, in addition to strong legs, will become crucial for momentum generation during sprinting. Now, it may happen that a competitor with excellent capabilities, and who is 70-75 kg – i.e. of average weight – can, for example, in barbell squatting, strengthen his muscles so that he can do squats or even series of squat jumps, even with a weight of up to 150-160 kg plus. His muscles are in great shape, his strength is still increasing, but at the mechanically vulnerable points, micro-injuries can begin to form: unnoticed wear, tears, and cracks. This does not necessarily occur later on in the observed and protected knee joints, but it may be that one of the intervertebral discs of the lumbar vertebrae will suffer permanent damage, for example. The competitor has a series of successes in his races for a few years and then his condition suddenly worsens as his spinal injury becomes such that he has to stop racing completely, or even has to change sport. Therefore, the development of muscles should not be treated as the sole benchmark if development of the whole locomotor system is the goal – and what else would the goal be? One of the secrets of healthy joints – the easy-to-create basic condition – is a thorough warm-up. The other is a rational load – it is much more difficult to determine the extent of this, as it is dependent on the sport and the individual.
3.2. Accidents and joints: traumatic injuries
Common causes of joint injuries are simply the sprains, strains and tears caused by unintentional movements and other accidents. These injuries can occur in a wide variety of situations, and can instantly ruin training results which have been built up over a long period of time. In some sports that require sudden, powerful movements and changes of direction (football, handball, basketball, tennis, combat sports, etc.), they are more frequent. Avoiding them is almost impossible, so what we can do at best, is to gradually strengthen the joints, and this is mainly the responsibility of the coaching activity of the given sport (for example, in order to avoid ankle sprains, that is, to strengthen the ankle ligaments, skipping is a tried and trusted practice).
Of course, during the painless phase of the healing of acute injuries too, there is a particularly vulnerable period when there is a great risk of re-injury. However, it is perhaps psychologically easier to follow the recommended waiting time for the restart of the workout because the traumatic experience here is more vivid than in the cumulative micro-traumatic type injury, the injury-inducing movements are clearer and the athlete is more aware of the cause of the injury. Furthermore, the healing phase is generally – a priori – longer, and medical assistance is used to a greater extent.
3.3. Cold and the joints
For the sake of completeness, it should be mentioned that the joints are also the most vulnerable parts of our locomotor system from the point of view of the cold, that is, they can get cold relatively easily if we do sport carelessly in cold weather. All of us know that when we travel in a car, or on a train with open windows in the summer, and when we lean out of the window for a longer period of time, we may experience joint pain in some parts of the arm for a shorter or longer period of time. Well, in cold-weather sporting activity essentially the same thing happens: the joint catches cold. This poses a real threat only to winter sportspeople and it is the responsibility of both athletes and coaches to be well aware of this; in other competitive sports, it is a negligible danger. Athletes practising on their own with no coach, may still run the risk of joints catching cold; however, this is outside the scope of the present subject.
Nowadays, however, a commonly used device poses a real threat of both common colds and joint colds (and for everyone, not just for athletes): this is a cold caused by air conditioning equipment. In the heat of the summer, the permanent exposure of a joint to a cold airflow can cause joint inflammation, and can throw back your workout.
3.4. Damaged tissue in the joint
3.4.1. The articular ligaments
The most frequent injuries during sport are to the joint ligaments. These formations behave as described for the elongation of tendons (elongation, flow, tear). The cause of the injury is mostly the twisting and/or bending force on the distal side of the limb. The damage to the ligaments usually happens in three fundamental ways. Most often, the connective tissue bundles forming the ligament themselves stretch or break. Second, avulsion injuries, in which the ligament (or tendon, or joint capsule) pulls out a piece of bone, should be mentioned. This type of injury is especially common in childhood, as the tensile strength of the bone tissue is still much weaker than that of the dense connective tissue elements fixing the muscle and joints. Thirdly, a separation at the ligament-bone interface can also occur, but this is very rare because the interface is particularly strong (Bartlett 2005).
The most obvious symptom of ligament injuries besides pain is joint instability. In addition, a lack of proper alignment, changes in pressure, and even loss of proprioception in the area may occur. Athletes who are most exposed to ligament injuries are those who have previously been injured in their ligaments, who have relatively weak muscles, and those who have excessively loose joints (Bartlett 2005) . It should be noted that in our daily activities, it is possible to use our joints regularly outside the elastic, only-elongating deformation range (e.g. when working in a squatting position, as in the case of tilers and plasterers). In this way, we spend a lot of time in a statically overstretched position that causes the elongation of the ligaments, which reduces their flexibility and stabilizing power, and increases the chance of injuries occurring during sports (Katics, Lőrinczy 2010).
When elongated and when partially torn, resting and gradual fine loading help recovery. A complete rupture may require surgical intervention. During the operation, long strips of one or more intact ligaments are cut off and attached to the bone in place of the torn ligament to replace the lost functions. Healing, as described above, takes several months or even a half to one year, so such an injury can thoroughly ruin a competitor’s calendar.
3.4.2. Articular cartilage
In the case of overuse and accidents, the cartilage can also be damaged, as well as the ligaments. The cartilage can respond to frequent overuse with wear, which threatens to develop into chronic arthritis. One-off extreme applications of force can cause the cartilage to crack or pieces can even break off from it.
However, it is important what kind of cartilage the injury affects. For example, damage to the meniscus in the knee is a common injury. This is, in some respects, a more serious injury than injuries to ligaments, because the replacement of the broken piece of cartilage cannot be achieved satisfactorily. In this case, surgeons try to treat the injury by cleaning the joint, removing the broken parts and smoothing the sharp edges. In exceptional, special cases, an attempt may be made to resew the broken meniscus piece.
In rare cases, extreme trauma may cause the hyaline cartilage covering the bone ends to come off, but here healing is even more challenging than healing meniscus.
It should be noted that one of the most common types of joint injuries caused by non-sporting activity, but due to an inappropriate lifestyle, is knee injury due to overweight: worn cartilage and torn cartilage.
3.5. Our main joints and more common types of injuries
3.5.1. Ankle joint
In general, the most commonly injured joint in sports is the ankle, within which, in terms of frequency, ligament injuries rank first (Bartlett 2005). The joint (Figure 11) is formed by the fibula, the head of which forms the outer side of the ankle (medial malleolus; malleolus lateralis), the tibia, the end of which forms the inner side of the ankle (lateral malleolus; malleolus medialis), and the ankle bone of the tarsus (talus); the whole structure is stabilized by a strong ligament system (Figure 12).
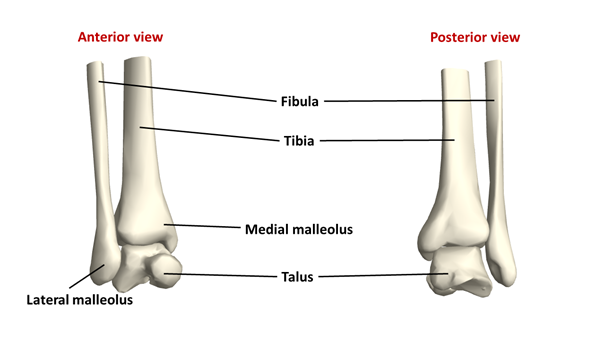
Figure 11: The ankle joint(Source: Wolfram Mathematica.)
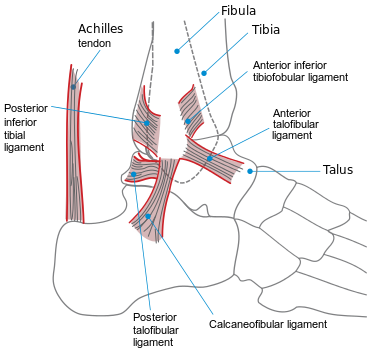
Figure 12: The ligament system of the ankle(Source: Wikipaedia. By An svg version of image:Ankle.PNG by me (Jak). Public Domain, https://commons.wikimedia.org/w/index.php?curid=1981086)
In the ankle joint a high mechanical tension is generated, as the foot forms a small load-bearing surface while the load is high. In the sole, the arrangement of its tiny bones creates two arches (Figure 13): a longitudinal and a transverse arch (the latter being in fact made up of the metatarsal bones). These two arches are of paramount importance from a biomechanical point of view, as they have a high energy-absorbing potential, i.e. they act as shock absorbers.
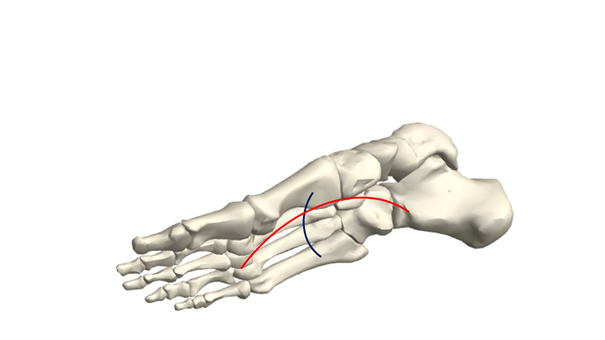
Figure 13: The biomechanical arches of the foot(Source: Wolfram Mathematica.)
In the ankle, alongside commonly occurring ligament strains and ruptures, inflammation of the tendon sheath (tendosynovitis) also occurs (in runners), and injury to the Achilles tendon is also common. This tendon is not typically an ankle joint element, but is discussed here because of its proximity. The tendon of the calf muscle, by which it is connected to the heelbone (calcaneus), is the Achilles tendon (Figure 8). Alongside the inflammation of its sheath and the adjacent bursa, this tendon is, unfortunately, torn relatively often, either by accumulating microtraumas or by a sudden impact (in sports involving jumping, sprinting, sudden changes of direction; Bartlett 2005).
Fractures (e.g. fracture of the lateral malleolus) are relatively uncommon injuries. Foot injuries are quite common, occurring about as frequently as ankle damage; roughly half of them are due to the accumulation of micro-injuries during overuse, and the other half are caused by one-off high-impacts in sports with a high risk of collision, or by a fall (Bartlett 2005).
3.5.2. Knee joint
In the highly complex knee joint, the femoral condyles (condylus medialis et lateralis) articulate to the tibia, to which the fibula is also connected from a lateral-posterior position (Figures 14-15). The kneecap is embedded in the tendon of the quadriceps femoris muscle (the tendon passes in the anterior portion of the knee and adheres to the tibia). The kneecap, in addition to its protective role, plays an important role in enhancing the effectiveness of the leg as a lever, since bypassing the tendon of the quadriceps over the joint, it increases the lever arm (Vogel 2013). The knee joint is also one of the most frequently injured joints in sport. Mechanically, it is subjected to forces from a wide range of directions, even during simple walking: bending, twisting, shearing (parallel to the joint surfaces) effects, and axial compression (Bartlett 2005). It is no coincidence, therefore, that the knee is relatively easily damaged during sports. Most often, the stabilizing ligaments (Figures 16-17) suffer injury: overstretching, partial tear or full tear. The latter injury mostly affects the anterior cruciate ligament, which, as we have seen, is one of the ligaments in the joint which heals with most difficulty in a spontaneous manner (Gabriel 2002).
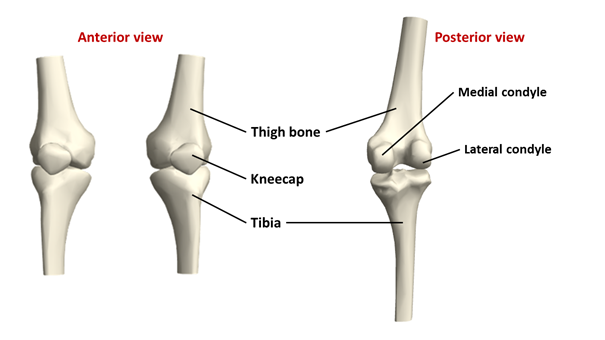
Figure 14: The bones of the knee joint(Source: Wolfram Mathematica.)
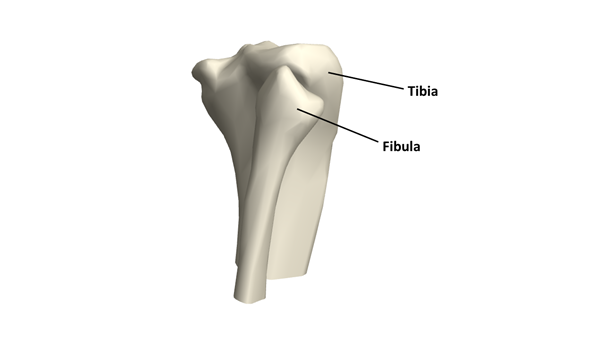
Figure 15: The relative positions of the upper parts of the fibula and the tibia (lateral and posterior view)(Source: Wolfram Mathematica.)
The tibia and the femur not only roll but slide on each other, so stabilization is needed in several directions, and is provided by the lateral ligaments, the cruciate ligaments and the menisci (Figures 16-17). The fibrocartilaginous rings of the meniscus absorb part of the energy generated during the impact which occurs when the foot hits the ground, and also play a stabilizing role in both an anteroposterior and mediolateral direction. In the case of knee injuries, a meniscus ring is often damaged by shear stress and compression: cracking or incidentally tearing. The common cause of meniscus injury is that we do a twisting motion with our body while the knee of the leg bearing the body weight is in a fixed hold (Bartlett 2005). Of course, meniscus injury can also occur due to overuse, but in this case it manifests more in wear, rather than in a rupture.
Traumatic knee injuries include damage caused by being struck, or kicked, and bursitis (bursa inflammation) caused by repetitive microtrauma, or inflammation of the kneecap tendon (patellar tendinitis), which mainly occurs in sports involving eccentric work exerted during repeated kicking off from a hard surface and returning to it (Bartlett 2005). This is the case in sports such as basketball, orienteering, football, or gymnastics.
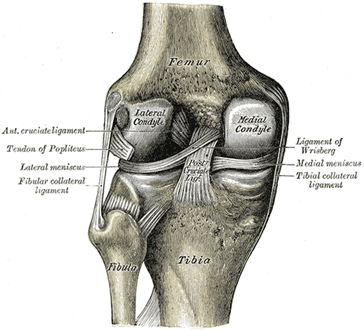
Figure 16: The ligaments and the menisci of the left knee joint from a posterior view(Source: Wikipaedia. By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See “Book” section below) Bartleby.com: Gray’s Anatomy, Plate 348, Public Domain, https://commons.wikimedia.org/w/index.php?curid=108270)
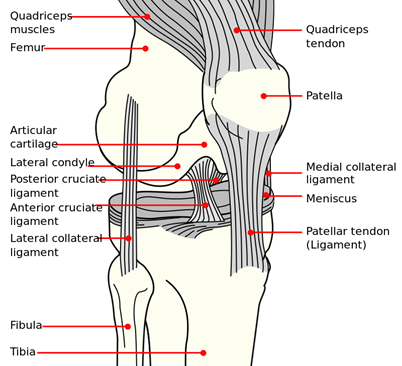
Figure 17: Anterior view of the ligaments of the right knee joint, drawn schematically. (Source: Wikipaedia. By Mysid - Vectorized and colorized in Inkscape, based on Image:Knee diagram.png., Public Domain, https://commons.wikimedia.org/w/index.php?curid=4004042)
3.5.3. The hip joint
The hip joint is the mobile, ball-and-socket joint between the girdle of the leg (the pelvic girdle) and the femur. The pelvic girdle is made up of the two pelvic bones – each fused from three bones: the ilium, the sitting bone (ischium), and the pubic bone (pubis) – and the sacral bone. In the pelvic bone there is a joint groove called the acetabulum; the head of the femur, or caput femoris fits into it (Figures 18-19). Its stability is ensured by a very strong ligament system (Figure 20).
Although the hip bones are largely formed by cancellous bone, they create a mechanically very strong structure due to their curved design. The freedom of movement of the thigh attachment region and the bending potential of the line of vertebrae, which individually is minimal, but taken together is significant, minimize the magnitude of the twisting and bending forces on the pelvic girdle (Bartlett 2005). Therefore, in sport, pelvic injury is quite rare. When it happens, it is usually due to the release of large compression forces resulting from collisions.
The most common fractures in the joint usually affect the femur, e.g. during a femoral neck fracture. However, the lesions of the muscle-tendon units (rectus femoris, adductor muscles, iliopsoas muscles) are much more common, and the inflammation of the pubic symphysis (symphysis pubica) through overuse also occurs in footballers, and more rarely in runners or long distance walkers (Bartlett 2005).
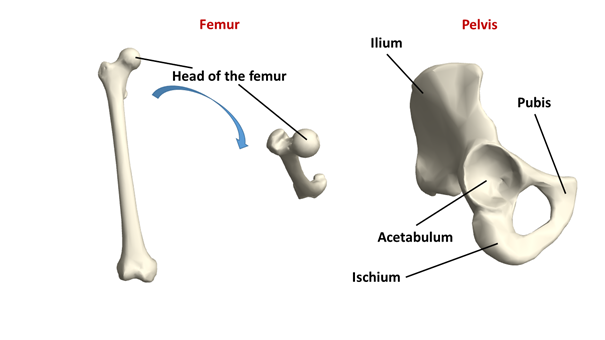
Figure 18: The thigh bone and pelvic bone joining in the hip joint (Source: Wolfram Mathematica.)
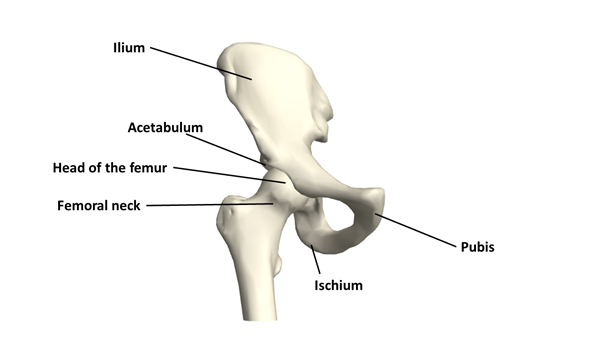
Figure 19: The structure of the hip joint(Source: Wolfram Mathematica.)
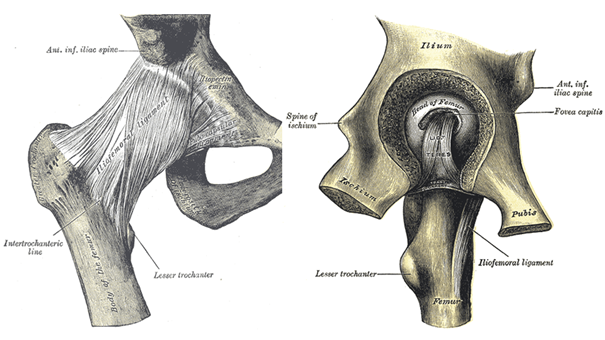
Figure 20: The hip joint is stabilised by a strong ligament system(Source: Wikipaedia. By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See “Book” section below) Bartleby.com: Gray’s Anatomy, Plate 339, Public Domain, https://commons.wikimedia.org/w/index.php?curid=108255;By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See “Book” section below) Bartleby.com: Gray’s Anatomy, Plate 341, Public Domain, https://commons.wikimedia.org/w/index.php?curid=108259)
3.5.4. The shoulder joint
The shoulder joint (Figure 21) is a very complex joint, which very often suffers injury. Its range of motion is large, but the price is that its stability is low, which is one of the reasons for the vulnerability. Consequently, the muscles around the shoulder are also necessary to maintain stability.
It is made up of the head of the humerus (caput humeri), the joint cotyle which holds it in the scapula (cavitas glenoidalis), the coracoid process (processus coracoideus) of the scapula, the bony process of the scapula which forms the edge of the shoulder (acromion), and because the collarbone also arrives at the acromion, and it joins to other structures of the shoulder joint with several ligaments, the clavicle is also a component of the shoulder joint. The head of the humerus forms a ball-and-socket joint with the cotyle of the shoulder blade, which causes the shoulder to have a large range of motion.
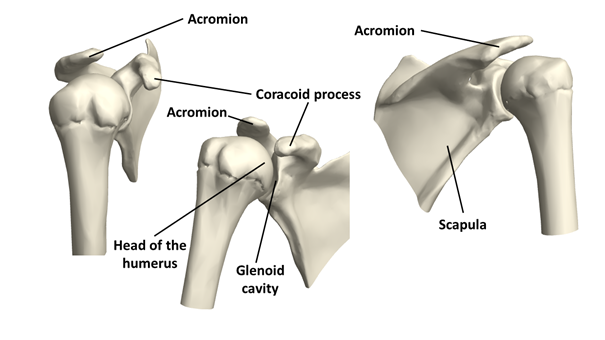
Figure 21: Articulation of the humerus and the scapula in the shoulder joint, from a lateral, an antero-lateral and a postero-lateral view(Source: Wolfram Mathematica.)
Some of the shoulder muscles (musculus supraspinatus, infraspinatus, subscapularis, and teres minor) form a collectively functioning group called the rotator cuff (Figure 22). The tendons of these muscles run between the head of the humerus and the acromion of the scapula. This area very often suffers injuries during sporting activity, especially when doing hard lifting, above-the-shoulder effort, various swinging and circular movements, and dynamic and large-diameter arm movements, which can cause both accumulative and one-off traumatic damage. Damage to the same moving unit and/or the acromion is caused by the axial pressure acting on the straight arm, pushing the head of the humerus upwards in the joint (Bartlett 2005).
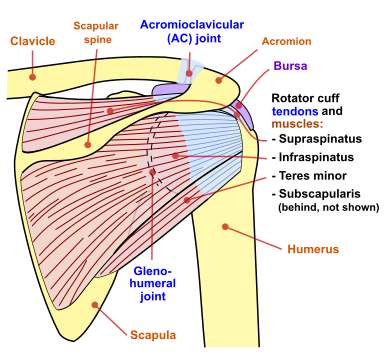
Figure 22: The tendons and muscles forming the rotator cuff (Source: Wikipaedia. By Jmarchn - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=67117834)
Another very common injury is the fracture of the clavicle, which may typically be due to falling on the shoulder or collision, i.e. a single traumatic damage. Otherwise, depending on the nature of the impact, the acromion, the coracoid process, the humeral neck, or the scapula may break (Bartlett 2005).
In addition to fractures, the dislocation of a component of the shoulder joint is relatively common: bone dislocation can occur either in the glenohumeral or acromioclavicular or sternoclavicular joints (Bartlett 2005). The inflammation of the bursa (bursitis), which is located under the acromion and protects the integrity of the tendons (Figure 22), is also a frequent shoulder injury, and is typically caused by repetitive overuse, just as is the inflammation of the tendon of the long head of the biceps (this tendon passes over the head of the humerus, and is attached to the scapula above the glenoid cavity, while the tendon of the short head is attached to the coracoid process; Figure 23).
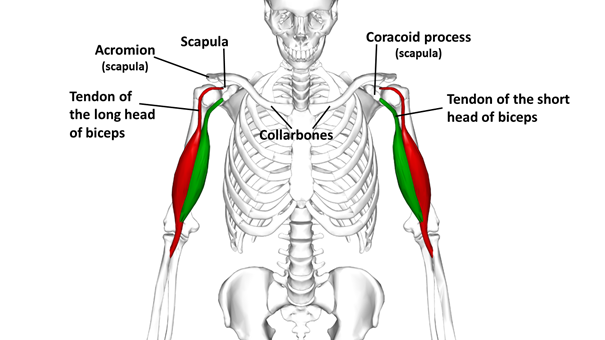
Figure 23: The location of the frequently injured bursa and biceps tendon within the shoulder joint(Source: Wikipaedia. By Anatomography - en:Anatomography (setting page of this image), CC BY-SA 2.1 jp, https://commons.wikimedia.org/w/index.php?curid=27449209)
3.5.5. The elbow joint
The elbow joint is the meeting of the humerus and the bones of the forearm. In this, on the one hand, the trochlea which forms the end of the humerus (trochlea humeri) and the articular fossa of the ulna (incisura trochlearis) are connected in a joint (Figure 24), on the dorsal side of which the olecranon can be found. On the other hand, the humerus’s “small head” (capitulum humeri) is attached to the proximal joint surface of the radius (fovea articularis). In effect, the articulation of the radius and ulna also belongs to the joint: the cartilaginous surface (circumferentia articularis) wrapping around the head of the radius (caput radii) fits into the radial notch, the articular depression on the ulna (incisura radialis).
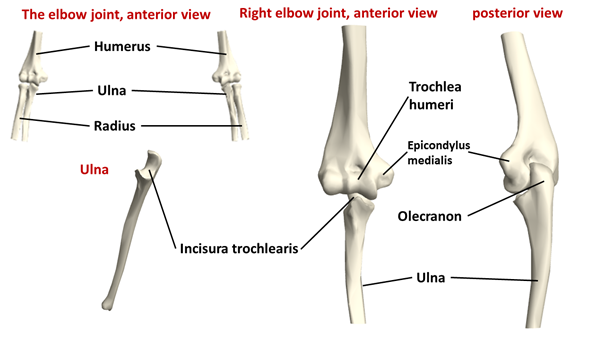
Figure 24: The structure of the elbow joint(Source: Wolfram Mathematica.)
During a fall, using the elbow for support may cause fractures of the olecranon, but a similar risk of breakage is present with hyperextension of the arm overstraining the triceps in throwing or striking movements (Bartlett 2005).
Elbows are affected by several symptoms stemming from repetitive overload. Tennis elbow (epicondylitis) is an inflammation of the periosteum as a result of the overstrain of the forearm’s extensor muscles, attached to the outside of the humerus (epicondylus lateralis; Figure 25), which can also be associated with inflammation of the tendons. Contrary to its name, it does not only occur in tennis players (and among them it is more likely to be caused by inappropriate technique and/or too many backhands), but can also be triggered by a variety of other physical activities, even including typing on a computer keyboard and mouse use, and carpenters, painters and butchers can also experience it. Golf elbow is a similar inflammation formed on the medial epicondylus of the humerus, which results from overstraining the flexing of the hands. Of course, it is not only golfers who are involved here, but also sportspeople doing other racket sports, as well as weightlifters, those doing throwing sports (e.g. javelin throwers), archers, and very often, of course, those who do not do any sport at all.
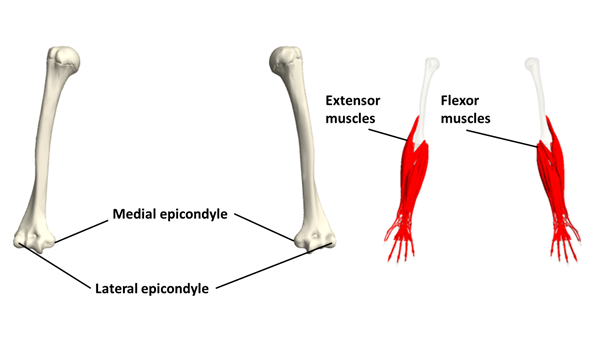
Figure 25: The attachment of the extensor and flexor muscles to the epicondyles of the humerus (with palms upward)(Source: Wolfram Mathematica.)
3.5.6. The wrist
In the wrist joint, the distal ends of the forearm’s radius and ulna meet the group of the tiny bones of the carpus (Figure 26). The wrist and the hands are also frequent sufferers of sports injuries, the trauma often occurring as a result of landing on the wrist when falling. Tendon sheath inflammations are also common in the wrist and in the hand (e.g. among those practicing tennis, squash, badminton, rowing sports); this is typically due to the additive effect of accumulating minor injuries. In contact sports, dislocation of the fingers also occurs. Wrist and hand injuries are typically more frequent in hand-dominated sports (apart from those mentioned above, basketball, rock and indoor climbing, golf, etc.; Bartlett 2005).
The bones of the hand create three biomechanical arcs: a longitudinal, a transverse and an oblique arc (Figure 27), which makes the hand capable of gripping objects with great force (Katics, Lőrinczy 2010). The skeleton constituted by tiny bones is stabilized by a plurality of ligaments and the extensive palmar aponeurosis, but due to their small size, both the bones and their joints are vulnerable to impact, twisting and pulling.
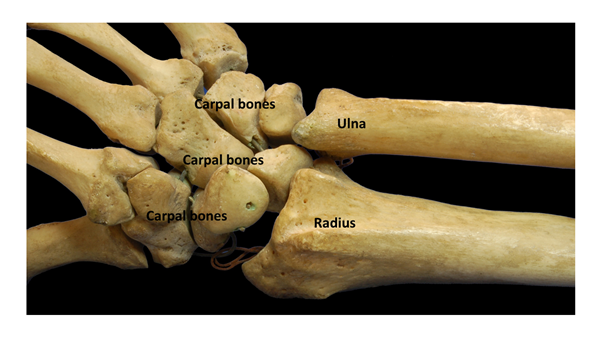
Figure 26: Structure of the wrist joint(Source: Wikipaedia. By Brian C. Goss - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=982489)
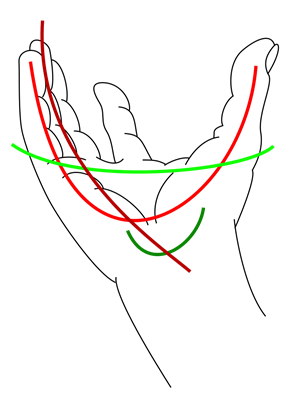
Figure 27: The biomechanical arches of the palm. The dark green line indicates a smaller, carpal arch, which, in terms of gripping capacity, forms part of the oblique arch indicated by the red line(Source: Wikipaedia. By Fama Clamosa - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=23508428)
3.5.7. Back and neck
The skull, with its vaulted structure, is able to withstand great static forces, as the external compression forces do not open but squeeze the sutures together (Katics, Lőrinczy 2010).
Traumatic injuries of the head are therefore caused by bumps, high-impact collisions and falls, in which a particularly large endangering factor can be their whiplash nature, in which the head behaves like the end of the whip, and, reaching the impact surface last, is forced to absorb high energy at impact, or is injured by being snapped quickly back and forth. Chronic head injuries are usually caused by the accumulative effect of blows received below the threshold of injury, such as those encountered in boxing, but similarly, by heading in football (Bartlett 2005).
The four curvatures of the spine – cervical forward curvature (lordosis), thoracic backward curvature (kyphosis), lumbar lordosis, and sacral kyphosis – ensure that the vertebral column, acting as a sort of spring, is able to absorb vertical forces (Figure 28). It is interesting that since lifting work forces the intervertebral discs to compress, the post-workout body height associated with such activity – e.g. among weightlifters – is less than when awakening because regeneration has not yet occurred. Likewise, disc collapse and weakening of the muscles in old age is the reason why the radius of the spinal curves decreases, and the body “shrinks”, i.e. loses its height (Katics, Lőrinczy 2010).
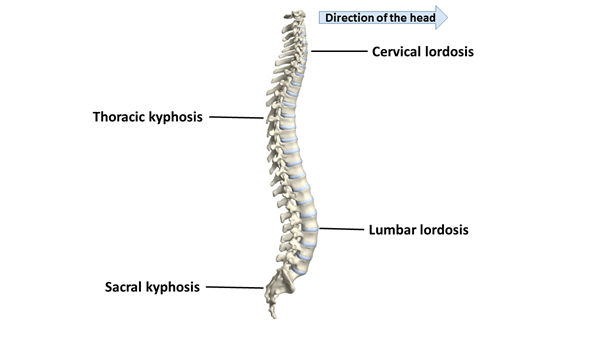
Figure 28: The curves of the spine(Source: Wolfram Mathematica.)
Spinal injuries are basically caused by over-bending or over-twisting movements, but in a fall, besides these, the compression effect can also occur. Neck injuries are mainly caused by heading type movements, but in combat sports, torsional damage due to joint locks is also present.
Excessive forward bending of the spine causes the vertebral body to compress while tension develops in the dorsal ligaments, but the bones of the vertebral body collapse before the damage occurs to ligaments, because the force acting here is three to four times the tension in the posterior ligaments (Bartlett 2005).
The injuries of the spine occur mostly at the border of the more mobile and rigid sections (Katics, Lőrinczy 2010). These include the cervical, thoracic and lumbar regions, all of which are prone to injury due to torsional forces. The 10-12th thoracic vertebrae react especially sensitively, and are vulnerable to sudden twisting movements because they are located at the border of two regions of mechanically high torsional stiffness (Bartlett 2005). Underneath are the lumbar vertebrae, which are also positioned in this vulnerable section, and although their vertebral bodies are the largest of the individual vertebrae (i.e. apart from the fused sacral vertebrae), they form a part of the axial skeleton that does not find support and force displacement in any other bony structures, so both twisting and bending movements can acutely damage them. In addition, lower back pain affects not only sportspeople, but also a great proportion of the non-sporting population. Spinal injury accompanied by lower back pain is quite easily caused by the following load types (Bartlett 2005):
Weight loads causing bending, e.g.
- lifting objects, for example weightlifting in sports;
- sports with repetitive bumps and jolts, e.g. running, riding.
Twisting effects, e.g.
- racket sports (tennis, squash, ping pong, badminton, golf, baseball);
- throwing sports (discus, shot put);
- sports that include aerial movements involving twisting of the torso (gymnastics, high diving).
Effects caused by arching backwards, e.g.
- volleyball, rowing, breast and butterfly strokes.
Since spinal integrity in all sports – and not just in sports – is key; in several sports regular spine exercises are used to maintain it.