7. Factors affecting the development of injuries
7.1. Sex
The bones and the entire locomotor system of the female and male body show significant differences in statistical averages. As a result of male hormones, a higher bone density, as well as a greater bone mass and musculature develop in adolescence. In women, the smaller bones, the lower muscle ratio and the higher body fat ratio, therefore, makes the body fit for fundamentally different types of load compared to men.
However, in addition to these size and mass differences, differences in proportions can also be observed. The structure of the female pelvis differs significantly from that of the male pelvis, which is not surprisingly the basis of the ability to carry the foetus. In the average female pelvis, the wings of the ilium are divergent, and the entire pelvis is of a smaller and wider construction than men’s; the pelvis minor (or lesser pelvis; the narrowest cross section through which the new-born baby’s head will have to fit) has a wide oval shape; the angle of the connection between the inferior rami of the pubic bones (angulus pubis) is obtuse, angled at about 120°. The sacrum is wide and flat. In contrast, the male pelvis is narrower and taller; it has steep iliac wings. The pelvis minor is somewhat triangular, the angulus pubis is around 90°, and the sacrum is pointed, arched, and spade-shaped. From this comparison, it can be seen that the constitutional differences in the pelvis create biomechanically different hip and knee loads in the two sexes, and through this, influence the movement of the whole body.
The performance values – measured in absolute numbers – achievable by the female organism (long distance times, top results in high jump, long jump, weightlifting, etc.) are therefore naturally lower on average than for men. However, in terms of injuries, the two sexes are by and large equally at risk. On the one hand, this can be explained by the fact that dexterity and coordination are roughly the same, and can be developed equally in the two sexes (Bartlett 2005). On the other hand, it may also be explained by the fact that – assuming appropriate warm-up, techniques and fitness – extreme sports activity is the most likely cause of injuries. And since extreme performance must be basically interpreted in relation to our own limits, the performance zone of high risk of injury is relative in this respect, and is, on average, equally valid for everyone.
To this theme, the concept of different weight categories can also be organically linked, which is an excellent analogy for understanding extreme sports activity and at the same time striving to increase competitive safety. Of course, it is now quite legitimate and reasonable to have matches within weight categories in contact combat sports (boxing, wrestling, judo, kick-boxing, Brazilian jiu-jitsu, etc.). However, in the earlier stages of sports history, this was not the case: everyone played with anyone who challenged or stood up against him/her. In this way, if a significant (e.g. 15-20 kg) weight difference existed between the competitors, the lower weight competitor was performing outside his/her comfort zone for the majority of the fight, while the heavier competitor was able to work within it for almost all the contest. So, what was, for the lighter competitor an extreme performance, for the heavier competitor was more likely to represent a normal, average fight load, with much less risk of injury than for the smaller opponent. Big differences in weight still occur in weight categories with no upper weight limit (heavy weight, super-heavy weight, ultra-heavy weight, depending on the sport). For example, boxers in the lower band of the heavyweight category in professional boxing are likely to choose this category because of the trophy rather than decide to lose a few kilograms and compete in the less prestigious cruiser weight for a lower purse. In addition to the compulsory protective equipment (e.g. mouth guards, gloves, men’s groin guards, and in the amateur sport, also shin guards and head protectors, etc.), the division into weight categories also serves to protect the competitor. Therefore, in modern combat sports there are fewer injuries per unit of competition time, and fatal matches are also much rarer than in the early days of fighting sports. As we have already mentioned, this is one of the reasons why there is no mixed sex competition in sports, especially in collision sports.
7.2. Training and competing in an unsafe performance zone: ambition and financial reasons
The problem with unsafe sporting activity may arise when we try to adjust our own boundaries to absolute performance values without realizing that we are no longer able to do so safely. Practice and competitive activities in unsafe performance zones can cause injuries of both an accumulative type, due to overuse, or an acute nature. It is a regrettable tendency, but in some respects it is perhaps understandable that in top level sport where the peak performances are produced, the goal is precisely to achieve absolute performance values and to break records. In attempting to achieve this, of course, the competitor’s individual best performance is also evolving, but if the pace of development is overdone and the goal is set too high, the health of the competitor will be harmed. In the most popular sports, huge sums of money are spent on the competitor’s salary and training, and if this is financed by private capital, the sports company in question automatically becomes profit-oriented. Of course, no training site, club, or “stable” openly declares that they will sacrifice the health of the competitor, if necessary, for the sake of performance and money, as this would be unlawful, but it emerges from the personal reports of professional athletes that we should be aware that this is very often the case in practice. In such systems, the competitor becomes a tool for making money.
Of course, the responsibility and competence of primarily the coach and the athlete is to judge the boundaries of the safe activity zone, but the psychologist professional can also help them, and warn them of the potential dangers, if he/she notices that the athlete, driven, for example, by ambition or other mental or material factors, may have gone beyond this zone, or be preparing to do so.
7.3. Age
Regarding age related risks of injury, first of all, it is important not to confuse the effects of age and inactivity on injuries (Bartlett 2005). However, even with constant physical activity, there are two riskier periods in human life in terms of injury: old age, and childhood, including adolescence.
At an older age, the athlete, of course, has to work more in his/her own maximum performance zone if s/he wants to maintain his/her previous level of physical condition and skills. As time progresses, this becomes increasingly difficult and then impossible, and if this is not recognised or taken into account by the individual, there is an ever increasing risk of injury. Injuries in old-age are mostly caused not by a single trauma, but by accumulative overuse, often as a culmination of degenerative-type processes. Therefore, tendonitis (tendosynovitis), bursa inflammation (bursitis), inflammation of the fascia (fasciitis) and inflammation of the joints (arthritis) are relatively common at this age. An important factor in the appearance of injuries in old-age is also that some of the injuries are caused by increased sensitivity due to damage at a younger age and the recurrence of injuries (Bartlett 2005).
In childhood and adolescence, the bones are not yet fully developed. Bones are formed from cartilaginous tissue in the process of ossification. Starting from the ossification centres within the bone, the ossified areas slowly expand, and gradually replace the cartilage. The process – considering the whole skeleton – ends around the age of 23. Then the bone mass still continues to grow, up to the age of about thirty. The long bones typically ossify from the diaphysis and the two epiphyses (Figure 29), so that in childhood the bone ends are not yet ossified to the body of the bone. The integrity of the epiphyseal growth plate is of paramount importance, as damage to it can lead to growth disorders. In addition, as discussed above, the tensile strength of bone tissue in this life phase is still lower than that of the tendons and articular ligaments, so the high-force, traumatic injuries that would provoke the joints to dislodge in adults often cause avulsion in children, i.e. parts of the bone are torn off. At a young age, the distal parts of the humerus, radius and femur are at severe risk from the point of view of injuries to epiphyseal growth plates, because in these regions the articular ligaments are attached to the epiphysis and not further up, to the zone towards the middle of the bone (Bartlett 2005).
In adolescence, during the rapid growth phase, muscle development usually does not keep up with bone lengthening, so the muscle-tendon unit is relatively short, which comes at the expense of flexibility; and this again increases vulnerability. In the light of all this, it is recommended that in childhood and adolescence, collision sports and extreme intensity training be avoided (Bartlett 2005).
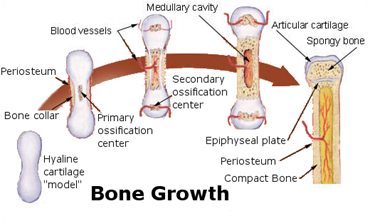
Figure 29: The process of bone formation(Source: Wikipaedia. By derivative work: Chaldor (talk)Illu_bone_growth.jpg: Fuelbottle - Illu_bone_growth.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=4353671)
7.4. Imbalances and anomalies of the skeletal system
The consequence of injury to the locomotor system of the lower limbs of different lengths is wear and inflammation due to overuse, and it causes excessive rolling of the foot inwards or outwards, and is typically associated with back pain and lower back pain.
If the angles between the femoral neck and diaphysis (angulus femoris) differ from the normal, this can cause a decrease in function in the (abductor) muscles of the hip, and also affects the inclination of the knee and foot (an “O-leg” or bowed leg, or an “X-leg” or knock-knees). The relative angular deviations of the tibia have similar consequences.
One of the static problems of the foot is flat feet (pes planus), in which the camber of the sole is not correct, and so it is flat. It also causes many locomotor injuries. It may result in dysfunction of the sacro-pelvic articulation, knee pain, carpal fractures and other accumulative problems, so it typically evokes an overuse injury profile.
Too high a foot arch (pes cavus, pes excavatus) is also a static anomaly of the foot, and can cause problems such as irritation of the lateral knee ligament, metatarsal fracture, peroneal tendonitis or inflammation of the plantar aponeurosis (fasciitis plantaris) (Bartlett 2005).
7.5. Physical fitness and training habits
It may well be trivial information that could also logically follow from our daily experience and knowledge, but we mention it because of the prevalence of the phenomenon: a lack of fitness, especially when combined with high body weight and high body fat ratio, significantly increases the chance of injury. This phenomenon often occurs when people who are substantially overweight want to lose weight abruptly, and introduce sudden and radical changes to their lifestyle. One element of this used to be to start some type of workout, such as jogging, weight training, etc. The danger is that with a significant amount of overweight, any training should only be started with great caution, and gradually, because it creates a sudden and disproportionately great burden on the joints. However, many people do not strictly adhere to this principle, firstly because they do not know about it, and secondly, because they do not take it seriously enough. For example, if you start jogging with a weight gain of 20-30 kg, and do not adopt a careful, gradual approach, you are likely to injure your knees and backbone quite quickly, as the rate of adaptation of the joints to sudden stress increases is limited. In this case, the injury will immediately stop the weight reduction process that has just begun, and the individual will easily return to his/her previous lifestyle, although just a small change in the training method would be enough not to hinder weight loss. When there is a lot of excess weight it is advisable to start weight loss from the nutrition side, and only later to burden the joints, or to choose an activity that causes little – weight-related – burden on the joints (e.g. swimming).
Another important influencing factor is the looseness of the elements of the locomotor system. Optimally loose muscles and joints protect against injuries, but excessive tightness and excessive looseness of the locomotor system both carry the risk of injury. However, there are differences of opinion regarding the setting of the optimum relaxation-stretching rate and the range of looseness; in any case it is generally accepted that loosening up exercises have a heightened importance in preventing, or reversing, the natural, spontaneous reduction in the movement range of the joints which takes place during ageing.
Another factor related to fitness is the strength of the muscles and the relative balance of their strength. For example, strains in the biceps femoris muscle occur at a higher rate if its strength is less than 60% of that of its antagonist, the quadriceps femoris; and even a 10% imbalance between these opposite side muscles carries a risk of injury (Bartlett 2005). This condition, unless there is an inherited muscle asymmetry in the background, can only be caused by specific strength exercises, i.e. by exaggerated, and usually isolated, strengthening of a muscle or muscle group, to the disadvantage of other muscles. This phenomenon, for example, poses a threat in bodybuilding where isolation exercises with machines can focus too much on the development of a single muscle, and the athlete ignores the fact that the elements of the locomotor system work together, in harmony, to make movements, so it is not advisable to overdevelop a muscle at the expense of the others, nor to exercise it in isolation. In addition to this, the phenomenon of muscle asymmetry occurs mainly in sports where one-sided movements and postures are predominant, such as canoeing or fencing. In such sports, great emphasis should also be placed on strengthening the muscles of the unworked side, but in these cases the dilemma arises as to whether to sacrifice valuable workout time to the detriment of further refinement of techniques, or further development of the active body side. The problem of training imbalances requires special attention especially in childhood and adolescence, since the locomotor system is still highly plastic, therefore it is easier to reverse any harmful processes, and at the same time – through faulty development – to also induce long-term locomotor anomalies.
One of the most important causes of injury is training errors. Misallocation of the training schedule and/or training workload usually results in local muscle weakness, which in turn impairs the shock-absorbing capacity of the muscle. This can then lead to accumulative stress injury in the bone or similar damage to the ligament system (Bartlett 2005).
Examples of training method errors include:
repetitive use of training sessions of too high intensity,
a sudden change in exercise intensity or load
a too monotonous workout plan (this is also not effective for performance, because the body quickly adapts to a certain type and volume of load),
incorrect or insufficient warm-up,
too little rest time between training sessions
returning to the activity too quickly after injury or inactivity (Bartlett 2005).
The combination of excessive training intensity (overwork) and the use of too little regeneration time is called overtraining. A typical overtrained athlete will:
produce results which reach a plateau phase and cannot improve,
be chronically tired,
continually perform below his/her personal best,
show the mental signs of burnout,
experience deterioration in coordination,
have an increased resting heart rate,
have an impaired heart rate recovery time,
lose weight,
lose appetite,
have muscular and joint pains,
have problems with sleeping,
have frequent illnesses,
have reduced self confidence,
have previously unexperienced emotional swings,
show symptoms of depression,
have reduced stamina,
and, in addition, can experience changes in many physiological, biochemical and immunological parameters (Radák 2016). Overcoming this condition can be greatly facilitated by help from a professional psychologist.